
California Drug Rehabs Face the Toughest Commercial Billing Scrutiny in a Decade
California drug rehabs face commercial billing scrutiny from four directions in 2026: pre-payment audits, SB 855 parity-driven review tightening, Marketplace authorization narrowing, and state enforcement around patient brokering. Compliant operators need tighter documentation, defensible coding, and audit-ready records to protect revenue.
5 Financial Blind Spots Costing Substance Use Rehabs Thousands

Behavioral health clinics rarely fail because of missing data. They fail because the reports they read are technically correct but operationally misleading. Gross overstates earnings, cash collections lag, a single NCR hides payer-specific bleeding, census outpaces AR aging, and standard buckets miss contract underpayments.
How Manual Billing Quietly Drains Behavioral Health Clinics (And Costs More Than You Realize)

Manual billing in behavioral health looks affordable on the salary line and quietly absorbs cost everywhere else. Lost clinical hours. Dropped admissions calls. Slower cash. Higher denials. Here is what the staffing math actually looks like and where the real cost lives.
In-House Billing vs. CodeMax – What Behavioral Health Facilities Should Know
In-house billing teams in behavioral health average AR cycles of fifty to sixty plus days. Outsourced partners average thirty to forty. The performance gap between in-house and specialized behavioral health billing is real and measurable, and it shows up in cash timeline, denial rates, and net collections every month.
How Slow Verification of Benefits Timelines Hurt Florida Rehab Admissions and Revenue

Florida rehab admissions are decision-window events. A patient ready to admit on Tuesday may choose another facility by Thursday if verification of benefits has not cleared. The lost admission never shows up on a denial report. Here is where the verification time actually goes and how parallel workflows compress 48 hours into 6.
What 2026 Reimbursement Changes Mean for Behavioral Health Operators
January 1, 2026 brought the most consequential single-year shift in behavioral health reimbursement since 2016. A Medicare conversion factor split, three new CoCM G-codes, direct Medicare billing for MFTs and MHCs, two new behavioral health telehealth codes, and a 7-day prior authorization decision rule under MHPAEA. Here is what changed, who benefits, and what to do in Q1.
The 7 Places Behavioral Health Revenue Leaks, and How Your Team Misses Them

Behavioral health revenue leakage rarely shows up as one obvious billing failure. It compounds across eligibility, authorizations, undercoding, denials, underpayments, out-of-window services, and self-pay aging. Aggregate dashboards hide each one. Here is where each leak lives, why your team probably misses it, and the three moves that recover the largest share fastest.
Behavioral Health RCM vs. Revenue Operations: Why Billing Alone Isn’t Enough
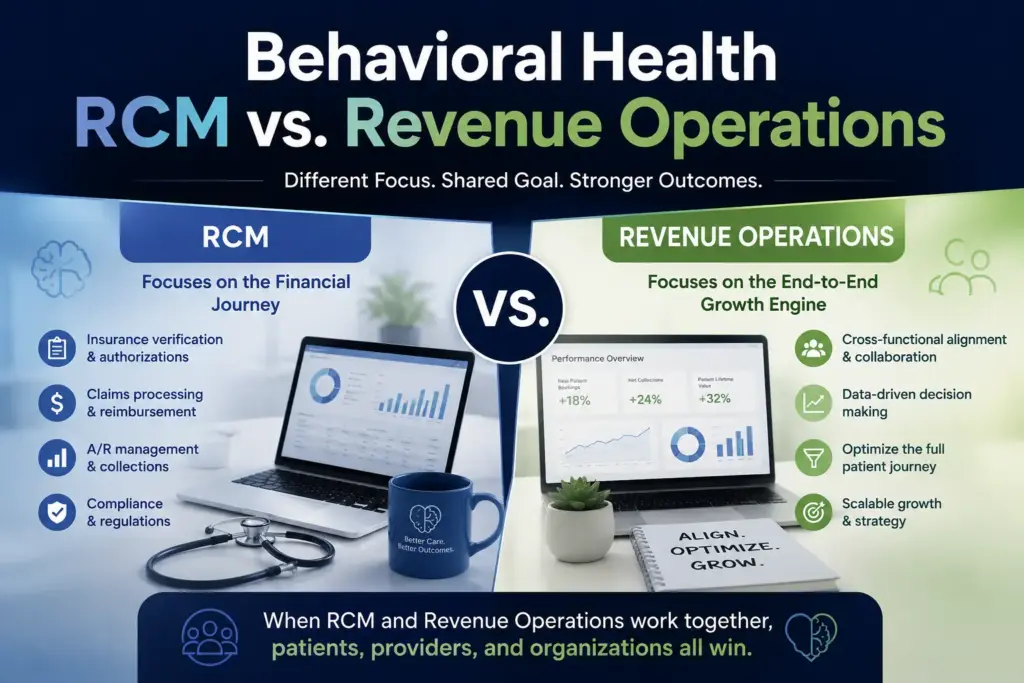
Behavioral health RCM and revenue operations are not the same thing. RCM is the transactional engine that turns delivered care into paid claims. Revenue operations is the strategic layer that decides what the engine should be running on. Facility leaders need both. Here is how to tell them apart and how they should hand off to each other.
Why California Rehab Centers Face Longer AR Cycles, and How to Close the Gap
California rehab centers commonly run AR cycles of 55 to 70 days, well beyond the HFMA national benchmark of 30 to 40. The cause is structural: 58 county Mental Health Plans, CalAIM code changes, telehealth modifier rules, and aggressive concurrent UR. Here are the five workflow disciplines that close the gap.
CPT Code 96372 in Behavioral Health: Denials, Dosing Errors, and Prevention Systems

Florida drug rehab billing breaks down in predictable ways. The transactional model that keeps a new treatment center running at low census stops working the moment the program grows. Here are the four places it fails, why Florida’s payer environment makes each failure more expensive, and what a billing operation built for scale actually looks like.
